
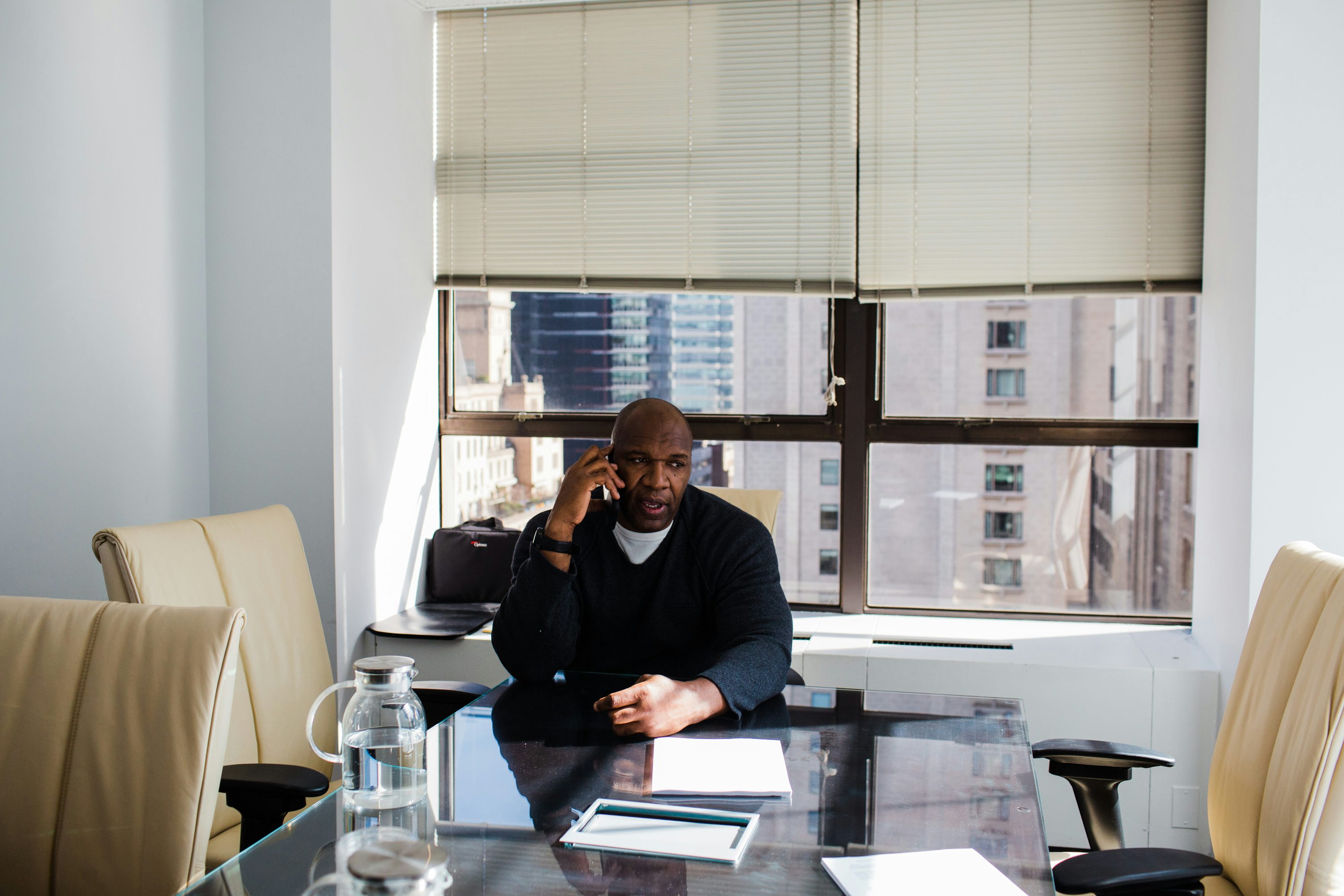
Photo by Benjamin Norman
The Marvin Washington Story: The Great Marijuana Mutiny Of The NFL
Opioid addiction and CTE are rotting the NFL to its core. Marvin Washington is a leader to an increasing number of football players who believe that medical cannabis can save players’ lives and, in many ways, the National Football League from itself.
Two years ago, Super Bowl Champion Marvin Washington received a message on Facebook from a former teammate. It read: “Marvin, I’m back living with my mom. I can’t function, man. I lost my wife and family. It’s a different deal. I’m taking nine pills of Percocet to just get through the day. Can cannabis help?”
Washington’s tone becomes unsettled when he recalls the situation. “The day before he called me, he was sitting in his mother’s kitchen thinking about drinking a bottle of bleach he saw in the laundry room.”
With 11 years in the league, Marvin Washington’s career is more than triple the average length for NFL players. Washington served as a defensive end for the New York Jets, the San Francisco 49ers, and the Denver Broncos, earning a Super Bowl ring in 1998. But to an increasing number of current and former players, Washington has become a vanguard for medical cannabis. He believes that opioid addiction and brain trauma are cancers metastasizing at the core of the NFL. Washington also believes that cannabis can treat them both.
Player Safety in the NFL
In the early 1900’s, football was on trial at The White House. Football had begun cementing its place in the national identity and drawing massive crowds on college campuses. But at the same time, the criticism surrounding its brutality and high rates of injury were mounting. Many were calling for it to be banned altogether. In the 1905 season alone, 18 college and amateur players were killed on fields across the country, mostly as the result of concussions, broken necks or internal bleeding.
Back then, football looked more like a blood sport than today’s gridiron. Players did not wear helmets, and they were only allowed to pass one another sideways. The result was violent takedowns, pileups and unrooted teeth on grass. So in the fall of 1905, Theodore Roosevelt assembled coaches from Ivy League schools across the country to discuss modifying the rules to save players’ lives and, in essence, save the game from itself. Many feared that modifications would ruin the game and discourage audiences who had become accustomed to its violence and fast pace. But opponents could no longer deny change was necessary after Union College halfback Harold Moore died of cerebral hemorrhaging in November of that year. The forward-pass was instituted. And the game didn’t die—it thrived.
“People say I am trying to kill football. I love football. I’m only trying to make it safer,” Washington says. Washington, who now works for cannabis-based medicine developers Kannalife and Isodiol, believes that today’s health crises in the NFL call for a similar paradigm shift.
“Football has a safety issue that the NFL is not addressing. There are 20,000 former players out there. We still represent the shield even when we are retired, but we can’t represent the shield when a lot of our brethren are incapacitated, living with their mothers, unable to work, unable to do anything because of opiate addiction or because of CTE,” says Washington.
Much like the black-lung-ravaged communities of coal miners, Chronic Traumatic Encephalopathy (CTE) and opioid addiction are industrial diseases of the NFL. Former NFL players misuse opioids at a rate three times higher than the general population. Further, CTE–a neurodegenerative disease resulting from repeated mild head injuries–is found in 87 percent of the examined brains of deceased football players.
Over the past several years, former NFL players have been increasingly coming forward to criticize the NFL’s policy on marijuana with personal testimonies about how the plant—or derivatives of its compounds known as cannabinoids—have significantly benefited their health. This begs the question: with player health at the forefront of conversations surrounding the NFL and steadily declining rates of participation in high school football, why is the NFL still enforcing its ban on cannabis?
As an athlete, Washington thinks the stigma of the couch-locked stoner plays a part. “Everyone thinks we are talking about rolling players blunts and sending them home, but there are all types of different delivery systems,” says Washington. Mostly, Washington blames the Controlled Substances Act for the NFL’s ban on cannabis.
So, Marvin Washington is suing the DEA and Attorney General Jeff Sessions to end cannabis prohibition.
Plaintiffs’ Memorandum of Law in Opposition Washington et al. v. Sessions et al. by Tyler Fyfe on Scribd
Marvin Washington et al. v. Jeff Sessions et al.
Joining Washington in the lawsuit are Alexis Bortell, a 12-year old with intractable epilepsy, Jagger Cotte, a 7-year old with Leigh’s Disease, Jose Belen, a veteran with PTSD, and the Cannabis Cultural Association, a non-profit helping underrepresented communities participate in the legal cannabis market. Named as defendants in the case are Attorney General Jeff Sessions, The Department of Justice, Acting Director of The Drug Enforcement Agency Chuck Rosenberg and the DEA.
Since the 1970s, cannabis has been classified as a Schedule I drug, the most restrictive category on the Controlled Substances Act which holds that cannabis is highly addictive and has no applications as a medicine. According to the plaintiffs’ attorney Lauren A. Rudick: “The classification of cannabis under the Controlled Substances Act was racially animated and infused with the desire to suppress political rights as opposed to having anything to do with public safety.”
In 1972, a commission appointed by then-President Richard Nixon famously told Congress that they should decriminalize marijuana possession as it showed some therapeutic potential and did not pose a major threat to Americans’ health. The White House decided to ignore the commission’s report, and the Domestic Policy Chief John Ehrlichman later told Harper’s magazine that the Nixon administration maintained prohibition as a way of rounding up blacks, hippies, and others consider a threat.
In the current political environment of the NFL—where players are taking a knee to protest institutional racism—this fact is significant. Between 2001 and 2010, black Americans were four times more likely to be arrested for marijuana possession. Between 2010 and 2014, they were three times more likely than white Americans to be killed by police. Seventy percent of NFL players are African-American, and for many like Washington, the acceptance of marijuana in the league is deeply personal.
Besides racial motivations, Washington et al. vs. Sessions argues that the Schedule I classification of cannabis violates the constitution on multiple grounds. Notably, the case argues that federal prohibition is in violation of the due process clause—that Americans are being denied the freedom to use life-saving medication on irrational grounds. Should Washington’s case succeed, the NFL would be forced to reconsider their substance abuse policy.

Medical Marijuana: The NFL’s Substance Abuse Policy
On November 29, 2015, Seantrel Henderson was in Kansas City, hunched forward on astroturf. As an Offensive Tackle for the Buffalo Bills, every Sunday, Henderson takes the yard line among a wall of face cages and eye black. At 330 pounds and 6-foot-7, Henderson was by all appearances indestructible. But those close to him at the time knew differently. Henderson had recently begun to suffer waves of searing pain in his stomach that would leave him nauseous and shrunken.
Two weeks later, he was rushed to a hospital in Philadelphia where it was discovered that two and a half feet of his large and small intestines were festering with disease. After an emergency surgery removing 80 centimeters of his intestines, Henderson was later diagnosed with Crohn’s Disease. For the next three months his bodily waste left through a hole in his abdomen collecting in a fitted pouch that needed to be emptied five to eight times per day. Fifty pounds of muscle withered and then disappeared.
Eight months later, after a second surgery to rearrange his organs, Henderson returned to training camp after regaining 20 pounds. But his comeback was short-lived. In September 2016, Henderson found himself suspended for four games for violating the NFL’s substance abuse policy. He had been using cannabis prescribed to him by a doctor to control the pain and nausea associated with Crohn’s. Despite clinical trials in Israel which had found that cannabis helped control the symptoms of 10 out of 11 patients with Crohn’s, in November of that same year, Henderson was suspended for a second time, for ten games without pay.
Brian Fettner, Henderson’s agent, says that until the next collective bargaining agreement between the NFL and the players union, “There is no medical provision for cannabis, even pill form.” CBD, the non-psychoactive cannabinoid derived from hemp oil, is also banned. The league does, however, allow a therapeutic use exemption for Adderall, an amphetamine prescribed for ADD known to be addictive and performance enhancing. The NFL also readily allows the dispensation of opioids.
While these facts combined with Henderson’s prescription might be cause for a legal battle in other industries, as a 9 billion dollar annual business, the NFL has nearly infinite resources for litigation. As contract workers, NFL players are keenly aware that the league has a monopoly on their dreams.
“Honestly no one has ever beat the NFL via a lawsuit that I know of. Not Tom Brady…no one,” Fettner said.
NFL teams appear to have put profit margins above employee health since at least the 1960’s. As football invaded living rooms across America, clubs began to value players for their ability to maintain viewers. In a sport where your muscles are shredded and then swollen, ripped and then bruised, your worth lies in your ability to take a hit and get back up again.
“The best ability that you have as a player is availability,” says Washington. “You have to be available to practice and play. If you are in the tub or the training room hurt, they count that as a black mark against you. So to get through practice, you do what it takes.”
Between July and January—or February if you’re lucky enough to make it to the Super Bowl—Washington tells me that many players submit to a routine of opiates and non-steroidal anti-inflammatory drugs prescribed by team doctors to cope with the pain from playing.
“Opiates are being pushed on you by team doctors, who are supposed to be looking out for you. But really they are the team’s doctor,” says Washington. “So they are going to say whatever they have to to get you on the field including pump you up with anti-inflammatories, opiates, and if you can’t sleep then benzodiazepines. That’s just the way it is.”
Doctors Are Urging the NFL to Embrace Cannabis
According to a survey by the NFLPA, of the players polled, 78 percent did not trust their team’s medical staff. “The reality is that they are on the payroll of the NFL and I think that it’s unlikely that they are going to bite the proverbial hand that pays their salaries,” says psychiatrist Dr. David L. Nathan.
Nathan grew up in Philadelphia among the residual tirades of reefer madness. Like most of his generation, he believed that marijuana was bad, that the people who used it were immoral and that the people who sold it were unworthy of their freedom. It was until after his residency at Harvard, during his years practicing psychiatry, that those assumptions completely collapsed. “I had seen just one too many cases of patients whose lives were ruined by a marijuana arrest when very few lives seemed to be ruined by marijuana itself,” said Nathan.
He soon realized that although most doctors he knew didn’t believe that cannabis should be against the law, very few were willing to speak about it publicly. So he founded Doctors For Cannabis Regulation, the first national physicians association dedicated to the legalization and regulation of cannabis in the United States.
In November 2016, DFCR penned a letter to the National Football League calling for the removal of cannabis from the banned substance list. When the League didn’t respond, Nathan published it. Then, in August 2017, NFL commissioner Roger Goodell told ESPN that cannabis “does have an addictive nature. There are a lot of compounds in marijuana that may not be healthy for the players long-term.” To Nathan, the league is a microcosm of society at large. And like the Department of Justice, he says that the NFL Commissioners Office still clings to debunked science.
“While players are freely able to get opioids which are highly addictive and NSAIDS which can cause other health problems, a drug that doesn’t have those side effects is prohibited. And that’s just not unfair, it’s also irrational,” says Nathan.
Opioid Addiction In The NFL
Since high school, Grant Mattos had lived by a simple mantra: if you’re not on the field, you’re not being seen. Mattos, a former NFL wide receiver who played for The San Diego Chargers, Denver Broncos, and Tennessee Titans, says the fear of losing his place on teams pushed him to take opioids, anti-inflammatories and Toradol injections with little understanding of what the medication was or its potential side effects. While the types of medication have changed with passing decades—from Oxycontin to Percocet to Vicodin to Toradol—according to players like Mattos and Washington, the pressure to play through pain remained the same.
“By the time I played for [the University of Southern California], my opioid consumption was very structured. It was just a normal thing. There was no ‘I can’t play because I’m hurt.’ The attitude in football is that you won’t make the club if you’re in the tub. This pressure just intensified in the NFL,” Mattos recalls. “I would just get them from teammates or whatever prescription the trainer had. I never cared about the names of what I was taking, a lot of them I couldn’t pronounce. I just cared about the result.”
Humans have known about the pain suspending power of the opium poppy since at least ancient Mesopotamia. For just as long, we have known that it can be cripplingly addictive and toxically lethal. Inside the brains and spinal cords of all humans exist mu-opioid receptors meant to receive the body’s endorphins and stimulate pleasure. However, for whatever evolutionary reason, mu-receptors clasp the morphine molecule found in all opioids with the ease of a plug slipping into a socket. The result is overwhelming euphoria and the dissolution of physical pain. However, tolerance to the morphine molecule builds quickly, and soon the body demands more and more. Much like a racketeer that protects you and then extorts you, opioids exact revenge when you withdraw from the arrangement. If the life of a person swallowing a steady stream of painkillers is one of comfortable numbness, the withdrawal from opioids is physical and psychological agony commonly described as the worst experience of an addict’s life.
In 2007, the dream ended for Mattos. Knee problems derailed his career after just four years. “It just feels like you have been discarded. Since I was eight, every day it was the only thing I thought about. You get there and then it’s over in the snap of your fingers, and you’re left standing in the middle of the desert going “what the fuck just happened?”
And the desert is exactly where he found himself. Mattos was working as a bartender in a dive bar in East Las Vegas, purchasing opioids off the street and drinking excessive amounts of alcohol. After years of painkillers, players are expected to quit cold turkey upon retirement, but the reality is, for a lot of guys, the drug use doesn’t end with their final game. “There is an after effect. If you have grown used to the flow of opioids and have even a hint of CTE while going through an identity crisis, it is a perfect storm,” says Mattos.
A 2011 study on opioid abuse in the NFL, the largest study conducted to date, found that 52 percent of NFL players report using opioids in their careers. Of those, 71 percent reported misusing these painkillers.
Mattos recalls the day he was fired from his job and kicked out of his girlfriend’s place. He sat in his car, in what was now his ex’s driveway, consumed by silence. He hadn’t slept. He could feel the Nevada sun burning through the windshield as it rose. He looked at the garage door. Then, he looked at himself in the rear-view. He felt vacant. “The feeling was utter despair, you’re at the edge of a cliff, and you could jump off of it, and you wouldn’t care,” says Mattos.
He knew that it had gone too far. So a friend wired him money for gas, and he moved to Los Angeles. He slept on a couch until he got a job at Equinox Gym in West Hollywood. It was there that he met a yoga instructor that introduced him to medical cannabis.
Mattos had grown up in the D.A.R.E. generation, and much of what he had learned about cannabis through public service announcements was saturated with fear. For decades, the “gateway drug” theory had dominated popular thought, leading the American public to believe that cannabis use was a springboard that would inevitably end in track marks and treatment centers.
Now, studies increasingly show that the gateway theory is not only incorrect but that cannabis could be an “exit drug,” with applications as an adjunct treatment for those struggling with opioid addiction. A 2014 study conducted by JAMA Internal Medicine found that between 1999 and 2010, states with medical marijuana laws experienced an average of 24.8 percent less opioid-related deaths than states without medical marijuana laws. A 2018 study by the RAND Corporation, the most comprehensive of its kind, found that easy access to medical cannabis through dispensaries resulted in a 40 percent reduction in opioid-overdose deaths.
“The combination of yoga, meditation and cannabis brought me back to life,” says Mattos, who has now been opioid-free for several years. “It was the first time I was okay with being alone. It was the first time I could say I loved myself. [Cannabis] worked then and it still works.”
Medical Cannabis: The Exit Drug
Dr. Mark Ujjainwalla, a certified physician by the American Board of Addiction Medicine for 30 years, has witnessed firsthand, among hundreds of patients, that when he prescribes medical cannabis or CBD derived from hemp-oil, they use less methadone. He prescribes medical cannabis to his patients as an adjunct treatment to control the emotional and mental fallout associated with addiction. While he doesn’t believe that medical cannabis is a cure on its own, he tells me that it is a vital tool in his strategy for harm reduction.
“The medical professionals that say this is a bad idea are either team doctors who fear losing their jobs or they drank the Kool-Aid that marijuana is a bad thing,” Ujjainwalla says. “I did sports medicine for 20 years. I wouldn’t prescribe anyone opiates. Ever.”

Derivatives of the opium poppy were traditionally only used by doctors to treat soldiers during war or patients in palliative care. The reason was simple: those on their deathbed were not at risk of developing addiction.
Medical Marijuana For Pain Management
Dr. Sana-Ara Ahmed is an Anesthesiologist and Chronic Pain Medicine Specialist in private practice in Toronto. Four years ago, Ahmed was introduced to the endocannabinoid system and the idea that cannabis could be potentially used to treat pain. As a specialist in anesthesiology, the information was jarring. How could she not have known this before? But her story is not unique. Most doctors aren’t taught about the endocannabinoid system. What often surprises pain doctors even more is that the human body actually has more cannabinoid receptors than opioid receptors.
“Their archaic model of saying opioids are better because they are blocking the mu-receptor is false,” Ahmed says. “Blocking the mu-receptor is what I do as an anesthesiologist in the operating room so that I can cut you open.”
In 2015, Ahmed opened her own practice that focused specifically on using medical cannabis to treat pain. The idea isn’t new.
In fact, there are records going back to 2737 B.C. which show that the Chinese Emperor Shen Neng prescribed cannabis for rheumatism or inflammation. Further, using cannabis for pain has drawn scientific interest since at least 1899 when Ernest Dixon found that dogs did not recoil from pinpricks after inhaling cannabis smoke.
Current research suggests that cannabinoids balance the hyper-excitable state of pain. Research also increasingly suggests that cannabinoids have applications as an anti-inflammatory and an analgesic.
Ahmed says, however, that cannabis treats pain differently than opioids in that it doesn’t numb the body and allow it to push through injury. Thus, she hypothesizes that the NFL has a financial incentive to push opioids instead of marijuana, which might encourage players to rest when the league wants them on the field. “The [NFL] has monetized the concept of pain and taken advantage of people who are vulnerable,” she says.

Eben Britton played six years in the NFL—four for the Jacksonville Jaguars and two for the Chicago Bears. During his career, he suffered a laundry list of injuries: a dislocated shoulder, a herniated disc in his back, torn muscles and ligaments all over his body. After his shoulder surgery, Britton was prescribed opiates. Within three days, he began waking up in the middle of the night with chills, cold sweats and daggers in his gut. What was more concerning was that, despite the side effects of the pills, he felt he needed more.
Britton was raised by a holistic family more likely to reach for herbal remedies than pills. He came to cannabis like most people: joints passed under smothered patio lights in backyards. He returned to cannabis while still in the league—not like the curious teenager seeking an unfamiliar high, but as an athlete channeling his upbringing to find the most sustainable way to manage his pain. Due to cannabis Britton says he didn’t take another painkiller throughout his last two years with the Bears with the exception of the occasional Advil.
“As a football player, you are in a highly adrenalized state, where you are running on testosterone and cortisol because you are constantly preparing for battle. Really every other substance exacerbates this fight or flight state,” says Britton. “Cannabis really nourished me emotionally, psychologically, as well as physically.”
Britton’s experience on cannabis was so transformative that he co-founded Athletes for Care, a coalition of athletes from the NFL, NHL, UFC, Olympics and extreme sports to advocate for medical cannabis. He says that removing cannabis from the banned substances list would benefit the NFL more than it realizes. For one, he says, it would drastically reduce the number of lawsuits filed against the league by former players or their families. Two, Britton argues that football players present an incredible case study for the advocacy of cannabis as a neuroprotectant in real-time.
Cannabis as a Neuroprotectant: CTE and Suicide in The NFL
Chronic Traumatic Encephalopathy, more commonly referred to as CTE, is a progressive neurodegenerative brain disease that has plagued the image of the NFL since it was discovered in the brain of former NFL player Mike Webster in 2002.
Webster spent the last years of his life shrouded in controversy. According to an ESPN Profile, he’d get lost among the streets of his own neighborhood while on his way home and spend days sleeping in his pick-up truck with a blue tarp taped over the windshield. When Webster died in 2002 of a sudden heart attack, he was examined by a doctor who found tangled knots of tau proteins in the crevices of his brain. Other parts of his brain had shriveled completely. It was obvious. When a healthy brain and one with advanced stages of CTE are placed side by side, the difference is akin to a newly harvested grape compared to a raisin.

Leonard Marshall is a former defensive end who played in the league for 12 years for the New York Giants, the New York Jets and the Washington Redskins. In 2013, Marshall was diagnosed with signs of CTE after undergoing a series of brain scans at UCLA. In 2015, along with 5000 former players, he received a $1 billion settlement in a class-action lawsuit against the NFL for brain trauma.
“Players signed the willful contract. They know the risks to obtain the reward,” says Marshall. “But what he didn’t sign up for, and what owners need to understand, is he didn’t sign up for a severe case of head trauma. They didn’t sign up for that they may no longer be able to care for their children.”
As he speaks to me, Marshall often stutters, his thoughts moving into lengthy tangents that veer from the question. Patients diagnosed with CTE are subject to a variety of symptoms: confusion, memory loss, trouble speaking, aggressive behavioral issues. Recently, suicidal thoughts have been linked to CTE too.
Marshall’s tone becomes somber as he begins to speak of his friend Dave Duerson. After playing in the NFL for a variety of teams for a decade, Duerson served as an NFL retirement board trustee, processing multiple disability claims for former players. But Duerson was dealing with undiagnosed brain trauma and severe depression. On February 11, 2011, Duerson sent his family a text from his Florida home. He asked them to send his brain to the University of Boston to be studied by neurologists researching CTE. He then picked up a gun and shot himself in the chest.
Leonard Marshall is part of a growing number of athletes who report that cannabis and its derivatives, like CBD oil, have helped them control symptoms associated with regularly smashing helmets. “If I had known about this stuff a long time ago, it could have helped save many of the lives of my friends. I mean many,” says Marshall.

For 40 years, Dr. Lester Grinspoon was the senior psychiatrist at the Massachusetts Mental Health Center in Boston. He is now associate professor emeritus of psychiatry at Harvard Medical School. Over the years, Grinspoon has increasingly felt guilty about his love of watching football. As more publicity around brain trauma began to surface from the closet of the league, he was slowly beginning to feel like he was living in Rome during the days of the Colosseum, cheering in the stands as Gladiators inflicted damage to one another that might end later be lethal.
He felt he needed to do something. So in 2014, he wrote and published an open letter on VICE’s Motherboard to NFL League Commissioner Roger Goodell, encouraging him to support further research into the efficacy of medical cannabis as a CTE treatment. (As in most conditions, there is a limited number of rigorous trials backing up football players claims about medical marijuana for CTE, among other field-related conditions.)
“If I were going to play football, I would decide to take this, because it might have some protective affects. It certainly would have no deleterious affects,” Grinspoon said.
The belief that marijuana should be removed from the League’s banned substances list immediately goes like this: if the NFL waits for cannabis and its cannabinoids to survive the years of clinical trials required to prove its efficacy, players will just continue to suffer the debilitating affects of CTE with no possible treatment. This situation is further complicated by the fact that the drug’s Schedule I status federally means that it’s very difficult to get all the necessary government approvals to research it.
Last year, the NFL sent a letter to the NFLPA offering to partner on a study into the use of cannabis for pain management. Later in 2017, Dr. Allen Sills, the NFL’s Chief Medical Officer, told the Washington Post that research into medical cannabis was “really important.” Currently, no updates have been given regarding the methodology of this study or when it will take place.
The Future of Cannabis in the NFL
An NFL spokesperson told Herb in a statement:
“The NFL and NFL Players Association have comprehensive programs and policies addressing both PEDs as well as illegal drugs and substances of abuse. In that respect, we rely on independent medical advisors who regularly review the most current research and scientific data, and there is more to learn about cannabinoid compounds as they may relate to their potential treatment of acute and chronic pain. This is an area of research we are looking to develop further, along with the NFLPA, to determine whether those substances could be used as an effective and safe pain-management tool for players. Currently, however, our advisors have not recommended making a change or revisiting our collectively-bargained policy and approach related to marijuana and cannabinoids.”
The vast majority of NFL teams currently reside in states that permit medical marijuana, and yet players’ use of the plant is still denied. Meanwhile, the NFL is the wealthiest sports organization in the world that, in some ways, is akin to religion. On Sundays, it has usurped church for millions of Americans who take to Lazy-Boy pews, testifying and speaking tongues at every touchdown. As an iconic American institution, it is in a unique position to change the tired narrative around cannabis as a dangerous substance and become innovators in the history of healthcare. The question is: will they?

Herb Recommended Products:
READ MORE









